
New York / New Jersey Lipedema Treatment
Lipedema, also known as a painful fat syndrome, is a chronic disease, which is most common in females. It is very poorly understood and commonly ignored.
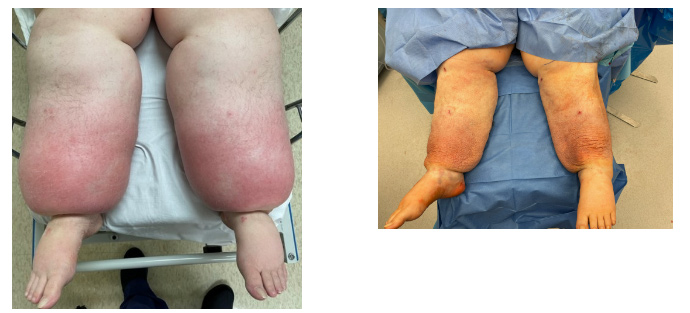





Power assisted, Water Assisted Liposuction combination treatment of legs below knees
immediate after surgery, no skin excision, 20L removed
Unfortunately, majority of doctors are not aware that this is a medical condition and commonly attribute excessive pain and fatty tissue accumulation in the lower half of the body and extremities to excessive weight and commonly recommend weight loss and/or bariatric surgery. Latest studies demonstrated that Lipedema is indeed a medical condition that requires treatment and will not improve with diet and exercise. Unfortunately, even bariatric surgery does not significantly improve Lipedema.
Vast Majority of patients who get lipedema are females but occasionally males can get it also. (Chen et al, 2004; Langendoen et al, 2009)
Exact incidence is unknown, but it is estimated that as many as 1% of US women can be affected by this condition. In UK it is reported 1 in 72000. (Child et al, 2010). In Germany, the prevalence of lipedema estimated at 11% in women and girls (Földi et al, 2006; Szél et al, 2014).
Power assisted, Water Assisted and Ultrasonic assisted L:iposuction combination treatment of legs below knees
3 month out no skin excision, 10L removed

Symptoms
Main symptoms of Lipedema include abnormal or excessive fatty tissue deposition in both lower torso, abdomen, hips, thighs, legs and occasionally arms. Feet and hands are usually spared and not affected by Lipedema. Symptoms also include easy bruising, increased sensitivity of skin to touch, cold feeling of skin and abnormally unpleasant feeling when somebody touches the affected areas, and pain. Pain may be accompanied by an unusual texture within the fat. Fat may feel like jelly or like rice, peas, or walnuts beneath the surface of the skin. Pain can also vary from none to severe, constant, come and go, or may only occur when the affected areas are touched, squeezed or pushed.

There is also a very significant psychologic effect on the patient. They are commonly uncomfortable undressing, or wearing more open type of clothing, which affects their self-esteem, establish family, and many activities of everyday living, such as ability to exercise, participate in public activities and family events, going to the beach, travel on certain forms of public transportation, like buses and airplanes, because of ability to fit in the seat or pain associated with it. Some patients getting tired very easily and have difficulty getting or maintaining employment. Some patients report difficulty getting in and out the vehicles.

Lipedema Cuffing. THIS IS NOT BEFORE AND AFTER IMAGE. THIS IS DEGREE OF CUFFING
There is a social stigma associated with having large lower part of the body, where lay people may associate Lipedema patients with laziness, uncontrolled eating habits, etc.
Cause
The cause of lipedema currently is unknown. First it was described in 1940 as a chronic incurable condition with abnormal accumulation of adipose tissues (Allen and Hines). The word Lipedema stands for “fat swelling”. It is also known under other names, such as Adiposalgia, Adiopoalgesia, Lipalgia, Lipohyperplasia, Lipohypertrophy dolorosa, Lipomatosis dolorosa of the legs, Painful column legs, Painful fat syndrome, Riding breeches syndrome and Stovepipe legs.
Most physicians believe that there’s a combination of genetic and hormonal factors involved in formation of Lipedema. Many patients report that several members of their family also have large legs on mother’s side. Studies also show up to 64% of patients report family members with this condition. Majority of our patient reports that lipedema usually starts at the point of significant hormonal stress, such as puberty, oral contraceptives use, pregnancy or menopause. It is also common that symptoms of Lipedema may get worse with age.
I believe that majority of lay people and physicians alike underestimate the complexity of Lipedema diagnosis.
Lipedema is not only excessive accumulation of fat. Most patients demonstrate abnormal formation of the lymphatic vessels in the affected areas also. No diet or exercise or bariatric surgery can fix that.
Nutrients and oxygen are delivered to lower extremities through the arteries. As the body consumes all nutrients and oxygen for its daily functions, the waste products are evacuated back to the body via two systems – veins and lymphatic vessels. Liver and kidneys then filter the blood.
Many of our patients with lymphedema experience abnormal function of veins and lymphatic vessels along with fatty tissue accumulation.
Instead of having normally functioning lymphatic vessels, patients with lipedema commonly have lymphatic vessels that are increased in size, loose, leaking or form small lakes (like aneurisms) where protein rich lymph accumulates.
With increased pressure inside of lymphatic system, lymphatic valves stop functioning normally and loose and dilated lymphatic vessels leak some of the lymph into surrounding tissues, which accumulate inside of the fat cells primarily. That is why the fat in the patients with Lipedema and Lymphedema does not look normal. It looks loose, watery, jellylike, and significantly whiter than a normal yellow fat. Other structures, like muscles, bones, tendons and ligaments, do no have ability to accumulate the lymph easily and usually not affected. Nerves, however, do get affected either directly or indirectly, when swollen fat puts pressure on them, resulting in increased sensitivity and pain.
Abnormal fat and lymph accumulation results in inflammation of the tissues and increased sensitivity. Blood vessels also become more fragile and may contribute to easy bruising.
As a patient accumulates additional fat in lower extremities because of genetics and hormonal changes, the fat cells progressively become bigger and bigger and also produce more waste products. At the same time there’s increased pressure on the main lymphatic channels in the area of the groins where it’s becoming more and more difficult to evacuate lymph from the legs.
In essence, it becomes a vicious cycle where the fat cells accumulate more fat and
more lymph, produce even more lymphatic fluid and cause stagnation, increased pressure, leak of lymph and prevents ability of lymphatics to evacuate lymph even more.
As the amount of waste products increases, the only other way to evacuate them is via venous system. Patients with lipedema commonly demonstrate abnormal function of the veins also resulting in venous insufficiency. The mechanism is similar to lymphatic system.
Therefore, in my mind, lipedema is not just a painful fat condition, it is a combination of abnormal function of the veins, lymphatic system and accumulation of painful fat.
Diagnosis
Majority of diagnosis is based on patient symptoms and clinical examination. Other studies, such as ultrasound, MRI, lymphangiogram and lymphoscincigraphy also can be useful.
Classic symptoms for diagnosing Lipedema include female patients, bilateral and usually symmetric accumulation of the fatty tissue below the waist, minimal pitting edema, pain, tenderness, hypersensitivity of the skin, easy bruising and feeling of cold on the skin. Usually, the feet are spared. The junction between the ankles and the feet may demonstrate excessive fatty tissue accumulation known as ankle cuffing.
In our practice I usually require the patients to undergo vascular ultrasound to rule out simultaneous insufficiency of the venous system in addition to lymphatic one. I approach Lipedema treatment in a comprehensive way. Diagnosis of venous insufficiency is challenging in Lipedema patients. Because of increased leg size, it requires quite a bit of experience to fully evaluate superficial vein function and not to miss improperly functioning venous valves. Performing venous ablation procedure (vein procedure) also requires additional skills and more advanced equipment then usual patients. That is why I prefer to diagnose and treat vein issues in lipedema patients in our office as we commonly have to redo the procedures from other doctors.
Treatment of Lipedema
Traditional treatments for Lipedema have very limited success. Usual recommendations include diet, exercise, nutritional modifications, emotional support, bio feedback, management of coexisting health conditions that may cause simultaneous leg swelling as well as complete decongestive therapy.
Complete decongestive therapy or CDT usually involves the combination of manual lymphatic drainage, compression therapy, use of customized compressive garments, physical mobilization as well as mechanical compressive devices to be used on a daily basis or continuously, such as Lymphapress. Unfortunately, despite all the above remedies, most patients experience very limited and temporary improvement.
Surgical options usually produce more long-lasting results. Studies demonstrated effectiveness of power assisted liposuction, waterjet assisted liposuction and ultrasonic assisted liposuction for reduction of the fatty tissue accumulation.
Excision of the affected skin with or without excision of underlying fatty tissue is also used.
Some surgeons also use manual extraction of painful nodules in addition to liposuction and excision.
Dr Volshteyn approach
Any form of liposuction that reduces the number of fatty cells in the lower extremities and other affected areas, also decreases metabolic demand on the tissues. It reduces ability to store excess lymph and overall reduces the amount of lymph traveling through the tissues.
Even though none of those surgeries restore normal function of lymphatic vessels, vast majority of the patients experience significant improvement of their symptoms and overall wellbeing.
Many of the patients that we see have very severe disease. It is not uncommon for me to remove over 20 pounds (or 10 L) of fatty tissue in a single session. Removal of traditional 5L recommended for cosmetic liposuction patients will not produce visible significant improvement. There are patients where I removed close to 80 pounds from lower extremities over several surgeries.

I use power liposuction to remove the bulk, water jet assisted liposuction to preserve lymphatic vessels and Ultrasonic liposuction to promote skin tightening after the procedure. The younger the patient, the better skin tightening is expected.
I used to excise the skin at the same time as the original procedure. Now I do it later and only if needed. I’ve noticed that many of my patients experience very impressive tightening of the skin when I use ultrasonic assisted liposuction (Vaser) which stimulates skin contracture. After about six or nine months, many of our patients do not require skin excision at all, especially below the knees.
Depending on extent and the severity of the disease, most patients require two or more surgeries separated by three months intervals of recuperation and rehabilitation. During that time, I recommend continued lymphatic massage, custom ordered garments and use of mechanical lymphatic devices, such as Lymphapress.
Patients who demonstrate venous insufficiency, also treated with either foam, laser, radio frequency devices or using a combination of techniques, in order to seal off faulty superficial veins.
Vein procedures can be performed in our office procedure room.

Click Here to see POWER ASSISTED LIPOSUCTION PROCESS
I do not perform high volume Lipedema surgery in the office setting because of concern for safety. Usually, I perform them either in the accredited licensed ambulatory surgery center or in the outpatient hospital facility.
Liposuction procedure is usually performed either under general anesthesia or sedation. Patients do not recall anything and do not hurt during the procedure. My procedures may take more time because I use several technologies simultaneously to achieve the best possible result.
After the procedure, a compressive dressing is applied, and patient resumes mechanical massage after 7-10 days after the procedure based on my protocol.
Skin excision is usually combined with one of the additional sessions.
Insurance Coverage
Many private plans do cover lipedema surgery based on the latest scientific studies. Aetna, Cigna and Blue Cross and others provide coverage for liposuction and excision surgery based on their internal policies. The process of authorization is time consuming and requires reports from primary doctor, or endocrinologist and possibly functional capacity evaluation. Despite that, my office had been successful in getting many of them approved.
Helpful Links
Lipedema foundation https://www.lipedema.org/
Fat Disorders Resource Society https://www.fatdisorders.org/
LipoedemaUK https://www.lipoedema.co.uk/
American Board of Venous and Lymphatic Medicine https://www.abvlm.org/search_instructions.php